Top Picks
Insomnia involves difficulty falling asleep, staying asleep, or waking too early with daytime impairment such as fatigue, poor concentration, or irritability. For some people it is short term, triggered by stress, travel, illness, or life changes. For others it becomes a longer-lasting pattern that affects daily functioning and overall health.
The options below are ranked using a consistent scoring lens: strength of supporting evidence, speed of relief, durability of results, safety and side effects, and access or cost. Each treatment follows the same structure to keep comparisons clear: what it is, who it helps most, how to try it, what to expect, cautions, and when to skip or seek guidance.
Some approaches may provide relief within days, while others require several weeks of steady practice. Safety considerations and underlying causes always matter, so expectations should match the type and duration of insomnia.
1. Pulsetto Vagus Nerve Stimulation
Best for: stress-related insomnia and bedtime hyperarousal.
Pulsetto is a non-invasive device designed to support vagus nerve stimulation, a method that may encourage parasympathetic activation and relaxation. The vagus nerve plays a role in regulating the body’s stress response, heart rate, and transition into a calmer state. For people whose insomnia is linked to racing thoughts, tension, or difficulty winding down, supporting this relaxation pathway can improve sleep readiness and may position it among the best sleep aid options for stress-driven sleep disruption.

Pulsetto is typically used 30-60 minutes before lights out. Sessions are short and structured. Users are encouraged to maintain consistency and track perceived calmness and sleep onset time over days to weeks.
What to expect: Some people notice improved relaxation within days, while others require several weeks of consistent use. It is not positioned as a replacement for clinical care but as a supportive bedtime tool.
Quick setup steps:
-
Choose a consistent pre-bed window
-
Run a short session
-
Track sleep onset time and perceived calmness
-
Adjust gradually based on comfort
Pros:
Cons:
-
Requires consistent use
-
Higher upfront cost
-
Not suitable without medical guidance for pregnancy, implanted electronic devices, seizure disorders, certain cardiac conditions, or neck sensitivity
2. CBT-I (Cognitive Behavioral Therapy for Insomnia)
CBT-I is a structured, evidence-based behavioral program designed to address the thoughts and habits that perpetuate insomnia. It is widely recommended as a first-line approach for chronic insomnia because it focuses on changing the patterns that maintain sleep difficulty rather than relying on ongoing medication use.
Insomnia involves difficulty falling asleep, staying asleep, or waking too early with daytime impairment. When this pattern becomes persistent, behavioral conditioning and unhelpful sleep beliefs often play a central role. CBT-I directly targets those mechanisms.
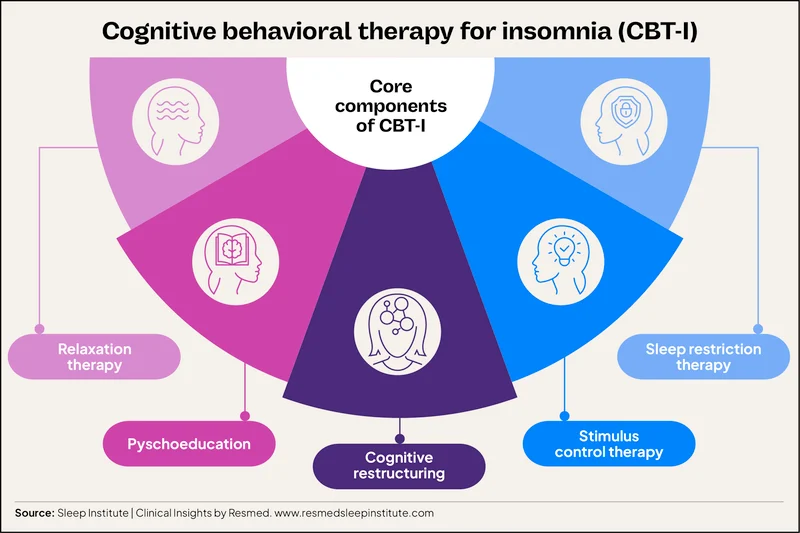
A standard CBT-I program includes five core components:
-
Stimulus control, which retrains the brain to associate the bed with sleep instead of wakefulness
-
Sleep restriction, which is time-in-bed management based on actual sleep duration, not sleep deprivation
-
Cognitive restructuring, which addresses worry-driven or catastrophic thinking about sleep
-
Relaxation training, to reduce physiological arousal
-
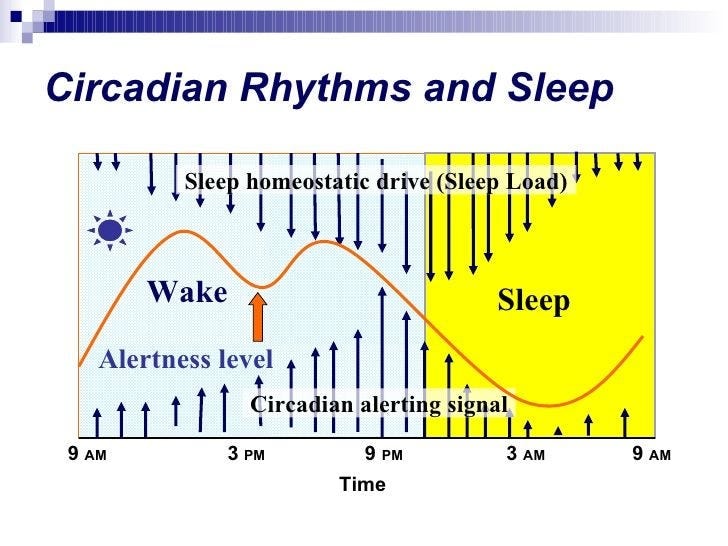
Sleep education, explaining sleep drive and circadian rhythms
Programs typically last 4-8 weeks. Improvements are usually gradual, with consolidation of sleep occurring over time. One reason CBT-I is preferred over long-term medication for many chronic cases is durability: skills learned during treatment often continue working after the program ends.
To begin:
-
Track sleep with a 2-week sleep diary before making changes
-
Set a consistent wake time and maintain it daily
-
Calculate average sleep duration from the diary
-
Set an initial sleep window close to that average
-
Adjust time in bed gradually based on sleep efficiency trends
Sleep restriction may temporarily increase sleepiness at first. Managing safety during this phase is important. If insomnia is severe, longstanding, or accompanied by significant daytime impairment, consultation with a clinician or referral to a sleep specialist is appropriate.
3. Sleep Hygiene and Bedroom Optimization
Sleep hygiene provides the behavioral and environmental foundation for improving insomnia. It rarely resolves chronic insomnia on its own, but it strengthens every other treatment by stabilizing sleep drive and circadian timing while lowering nighttime arousal.
The most impactful adjustments focus on consistency and light exposure. A fixed wake time every day, including weekends, anchors the internal clock. Morning light exposure within the first hour of waking reinforces that rhythm. Caffeine is best limited earlier in the day, and alcohol should not be relied upon as a sedative because it fragments sleep later in the night. Exercise supports sleep, but intense sessions are better scheduled earlier rather than close to bedtime.

Bedroom conditions matter just as much. Keep the room cool, dark, and quiet. Set clear screen boundaries and avoid stimulating content before bed. A predictable wind-down routine signals to the body that sleep is approaching. Understanding how to increase deep sleep begins with managing light timing, nervous system downshifting, and environmental consistency, which are explored further in this guide on how to increase deep sleep.
Common traps include weekend sleep-ins that shift circadian rhythm, alcohol used as a shortcut to sedation, and doomscrolling in bed.
Mini-checklist:
-
Fixed daily wake time
-
10–30 minutes of morning light
-
Afternoon caffeine cutoff
-
Reduced evening alcohol
-
Exercise earlier in the day
-
Cool, dark, quiet bedroom
-
Screens off before bed
-
Consistent wind-down cue
-
No work or scrolling in bed
Consistent application of these fundamentals strengthens sleep pressure and improves the effectiveness of more structured insomnia treatments.
4. Stimulus Control and Sleep Restriction Therapy
Stimulus control and sleep restriction therapy are two of the most powerful behavioral levers for conditioned insomnia and fragmented sleep. They are core components of CBT-I and work by rebuilding the link between your bed and consolidated sleep while strengthening natural sleep drive.
When insomnia persists, the bed can become associated with frustration, clock-watching, and alertness. Lying awake for long periods reinforces wakefulness in the sleep environment. Stimulus control reverses that pattern through clear behavioral rules:
-
Use the bed only for sleep and intimacy.
-
Go to bed only when sleepy, not simply fatigued.
-
If you are awake for about 15-20 minutes, leave the bed and go to a dim, quiet space.
-
Return only when sleepy again.
-
Keep a fixed wake time every day, including weekends.
-
Avoid naps, or cap them briefly if necessary.
These rules retrain the brain to associate the bed with sleep rather than prolonged wakefulness.
Sleep restriction therapy addresses excessive time in bed, which often develops when people try to compensate for poor sleep. The process begins with a two-week sleep diary. Calculate your average total sleep time and set an initial sleep window close to that average while maintaining a consistent wake time. For example, if average sleep time is six hours, the sleep window might initially be set near six hours. As sleep becomes more efficient and consolidated, the window is expanded gradually in small increments.
Short-term sleepiness is common in the early phase. This is expected as sleep drive rebuilds. Manage it safely by avoiding driving when drowsy and maintaining the fixed wake time even after a rough night. Consult a clinician before attempting sleep restriction if you have bipolar disorder, seizure risk, severe daytime sleepiness, or a safety-sensitive job.
5. Relaxation Training (Breathing, PMR, Mindfulness)
Relaxation training is designed to reduce physiological arousal that can delay sleep onset. Many people with insomnia describe feeling tired but mentally alert at bedtime. Techniques that gently lower activation in the body and mind can support a smoother transition into sleep.
Three evidence-informed approaches are commonly used:
Diaphragmatic breathing. Breathe slowly through the nose, allowing the abdomen to expand, then exhale fully and slightly longer than the inhale. A simple paced rhythm, such as four counts in and six counts out, practiced for several minutes, may reduce perceived stress and quiet racing thoughts.
Progressive muscle relaxation (PMR). Systematically tense and release muscle groups from head to toe. Hold gentle tension for a few seconds, then release fully before moving to the next area. This process helps increase awareness of muscle tension and supports physical unwinding.
Mindfulness or body scan. Direct attention to physical sensations or the breath without judgment. If the mind wanders, gently return focus to the chosen anchor. This can decrease cognitive hyperarousal that interferes with sleep.
Practice these techniques earlier in the evening rather than only at bedtime. A 5-10 minute session daily for 1-2 weeks allows the body to learn the pattern. If awakenings occur at night, use the same technique rather than switching methods.
For anxiety-driven insomnia, schedule “worry time” earlier in the day and keep notes outside the bedroom to prevent rumination in bed. Pair relaxation with dim lighting and a consistent wind-down cue such as quiet reading or calming audio. Some people also explore music and sound-based approaches that may help improve sleep as part of their evening routine.
6. Light Therapy and Circadian Rhythm Scheduling
Light is one of the primary signals that regulates circadian rhythm, the internal clock that influences when you feel alert and when you feel sleepy. Morning light exposure helps anchor that clock to a consistent wake time, while bright light in the evening can delay melatonin release and push sleep later. When circadian timing drifts, insomnia may show up as difficulty falling asleep until very late, trouble waking for morning obligations, or persistent grogginess.
Common signs of delayed sleep phase include feeling mentally alert late at night, struggling to fall asleep before midnight or later, and finding early mornings especially difficult. Irregular schedules and shift work can further disrupt circadian alignment.
Actionable timing strategies include:
-
Get outdoor light within 10-30 minutes of waking whenever possible, even on cloudy days.
-
Keep a consistent wake time daily, including weekends.
-
Dim indoor lighting 1-2 hours before bed.
-
Limit bright screens and overhead lighting late in the evening.
-
Shift sleep timing gradually in 15-30 minute increments rather than making abrupt changes.
Light boxes are sometimes used when natural morning light is limited, but people with bipolar disorder or certain eye conditions should consult a clinician before trying structured light therapy.
For shift workers, strategic exposure to bright light during the active period and intentional darkness after shifts can support adjustment. Managing light consistently over several weeks often produces steadier results than short, inconsistent attempts.
7. Melatonin (Targeted Timing and Dose)
Melatonin is a hormone that helps regulate circadian rhythm, the internal clock that signals when it is time to feel sleepy. It is generally more helpful for adjusting sleep timing than for acting as a strong sedative. For that reason, melatonin tends to be most useful when insomnia is related to jet lag, delayed sleep phase, or schedule changes that have shifted bedtime later than desired.
Timing matters more than dose. For circadian phase shifting, melatonin is commonly taken about 1-3 hours before the intended bedtime. Taking it in the middle of the night is usually not recommended unless a clinician has provided specific guidance. Many experts suggest starting with a low dose and following the product label rather than assuming higher amounts will work better. More is not necessarily more effective.
Possible side effects include vivid dreams, morning grogginess, headache, or gastrointestinal discomfort. Product quality can vary between brands, so looking for third-party testing and transparent labeling is important.
Caution is advised for people who are pregnant or breastfeeding, taking anticoagulants or immunosuppressants, managing seizure disorders, or using other medications. Children and adolescents should only use melatonin under medical supervision. If sleep difficulties persist despite appropriate timing and dose, further evaluation may be warranted.
8. Prescription Sleep Medications (Short-Term, Clinician-Guided)
Prescription sleep medications may be considered when insomnia is acute, severe, or significantly impairing daytime functioning. They are generally intended for short-term use and should be prescribed and monitored by a clinician. For many people, medication serves as a temporary bridge while behavioral treatments such as CBT-I begin to take effect, rather than a long-term standalone strategy.
Several categories are commonly used. Dual orexin receptor antagonists (DORAs) reduce wake signaling in the brain and may support both sleep onset and sleep maintenance. Non-benzodiazepine hypnotics, often called “Z-drugs,” are frequently prescribed to shorten sleep onset or reduce nighttime awakenings. Benzodiazepines are used more cautiously and typically only for brief periods due to higher risks of tolerance and dependence. Low-dose doxepin may be considered for sleep maintenance difficulties. Ramelteon acts on melatonin receptors and is sometimes used when circadian timing plays a role. In select cases, sedating antidepressants are prescribed when insomnia coexists with mood symptoms.
Potential benefits include faster sleep onset, fewer awakenings, and improved short-term sleep continuity. However, risks vary by class and individual factors. These may include next-day sedation, slowed reaction time, dizziness, cognitive impairment, dependence, tolerance, complex sleep behaviors, and increased fall risk in older adults. Interactions with alcohol or other sedatives can increase respiratory depression and accident risk.
Because of these considerations, clinicians generally recommend the lowest effective dose for the shortest necessary duration, followed by reassessment. Long-term use without monitoring is discouraged. Medication plans should include discussion of side effects, tapering strategies, and alternative treatments.
Candidates may include individuals experiencing acute severe insomnia, short-term life stressors, or those who need symptom stabilization while beginning CBT-I. People in safety-sensitive occupations should discuss next-day alertness concerns with their clinician. Avoid driving or operating machinery if residual drowsiness occurs.
Prescription sleep medications can be helpful in specific situations, but they require careful oversight. Ongoing evaluation helps balance symptom relief with safety and long-term sleep health.
9. Treat Underlying Conditions (sleep apnea, RLS, pain, depression, meds)
Insomnia is not always a primary sleep disorder. In many cases, it reflects another medical, hormonal, or psychological condition that disrupts sleep continuity. When sleep difficulties persist despite structured behavioral changes, it is important to consider whether an underlying contributor is present and to seek appropriate evaluation rather than continuing self-directed experimentation.
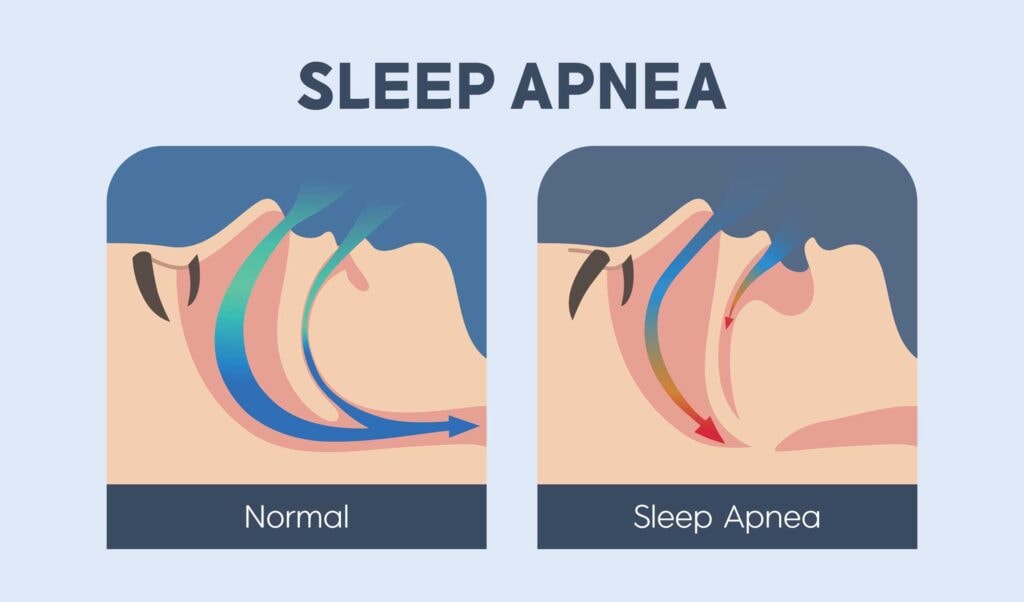
One of the most common contributors is obstructive sleep apnea. Warning signs include loud snoring, witnessed breathing pauses, gasping during sleep, morning headaches, dry mouth, and excessive daytime sleepiness. Some people with sleep apnea report difficulty staying asleep rather than classic sleepiness, and treating apnea can improve insomnia symptoms in certain individuals. Understanding how evaluation and treatment work can be helpful, including learning about best sleep apnea devices in the context of formal screening rather than self-diagnosis.
Restless legs syndrome may present as an uncomfortable urge to move the legs at night, delaying sleep onset. Chronic pain conditions can fragment sleep and prevent restorative rest. Reflux may worsen when lying down, leading to awakenings. Thyroid imbalance can alter sleep timing and energy levels. Anxiety and depression frequently coexist with insomnia and may require targeted mental health treatment. Substance use, including alcohol or stimulants, can disrupt sleep architecture. Hormonal shifts during perimenopause or menopause may also contribute to nighttime awakenings or difficulty falling asleep. Certain medications, such as stimulants, steroids, and some antidepressants, can interfere with sleep timing or depth.
Red flags that warrant medical evaluation include:
-
Loud snoring with witnessed apneas
-
Significant daytime sleepiness affecting driving or safety
-
Morning headaches combined with snoring
-
Worsening mood symptoms or panic episodes
-
Persistent insomnia despite consistent behavioral efforts
Professional assessment helps determine whether insomnia is primary or secondary and guides targeted treatment. Screening and clinician input are more reliable than attempting to diagnose underlying conditions independently.
10. Sleep Tracking and a 2-Week Insomnia Diary
Sleep tracking can clarify patterns that are difficult to see from memory alone. A simple 2-week insomnia diary often provides enough information to guide next steps without becoming overly complicated. The goal is not perfection, but pattern recognition that supports decisions commonly used in CBT-I and other structured approaches.
Track the following each day:
-
Bedtime and lights out
-
Estimated time it took to fall asleep
-
Number and duration of awakenings
-
Final wake time
-
Naps
-
Caffeine and alcohol intake
-
Exercise timing
-
Stress levels
-
Medications or supplements
After 14 days, review the data rather than reacting to single nights. Identify whether the dominant pattern is difficulty falling asleep, repeated awakenings, or early morning awakening. This distinction helps guide intervention. Sleep onset difficulty may suggest hyperarousal or stress-driven insomnia. Maintenance insomnia may reflect conditioned wakefulness or sleep apnea. Very late sleep timing may point toward circadian misalignment.
Wearables can help identify general trends, but they may misestimate sleep stages and overemphasize nightly scores. Prioritize overall patterns instead of individual sleep metrics. Over-tracking or obsessing about data can increase sleep anxiety, a phenomenon sometimes called orthosomnia.
Once a pattern is identified, choose one or two targeted interventions and apply them consistently for 2-3 weeks before changing course. Making multiple changes at once makes it harder to determine what is actually working.
How to Choose the Best Insomnia Treatment
Choosing among the best insomnia treatments works best when you match the approach to your insomnia pattern, how long it has been going on, and what seems to drive it. Start by separating acute insomnia (lasting less than a few weeks) from a more persistent, chronic pattern. Short-term sleep disruption often follows travel, illness, schedule changes, or stressful events and may improve with routine and recovery. Longer-lasting insomnia is more likely to involve learned sleep disruption, circadian misalignment, or comorbid symptoms that benefit from a structured plan.
Next, identify the dominant type:
-
Sleep-onset insomnia: trouble falling asleep, often linked to hyperarousal, worry, or a second wind at night
-
Sleep-maintenance insomnia: frequent awakenings or difficulty returning to sleep
-
Early morning awakening: waking too early with reduced total sleep time
Then ask what category fits best: circadian (timing shifted late or irregular), hyperarousal (stress physiology and racing mind), or conditioned insomnia (the bed becoming a cue for alertness rather than sleep). Also note comorbid symptoms such as loud snoring, restless legs sensations, pain, reflux, mood changes, or medication changes, because these can shape the safest next step.
A practical decision guide:
-
If insomnia is acute (under a few weeks): prioritize sleep hygiene and bedroom optimization, add relaxation training, and keep your wake time stable so the problem does not become conditioned.
-
If insomnia is chronic or recurring: CBT-I is the best supported approach for long-term change, and it often includes stimulus control and sleep restriction as core tools.
-
If stress or anxiety dominates: prioritize relaxation training plus stimulus control, and use Pulsetto as a supportive pre-bed routine to help downshift hyperarousal and improve sleep readiness.
-
If your schedule is late or irregular: prioritize light timing (bright mornings, dim evenings), a consistent wake time, and carefully timed melatonin for circadian shifting rather than middle-of-the-night dosing.
-
If loud snoring or daytime sleepiness is present: prioritize evaluation for sleep apnea rather than trying to “push through” with routines alone.
In general, behavioral approaches tend to be lowest risk and most durable, medications are usually best as short-term, clinician-guided support, and devices or routines can be useful add-ons that improve consistency without replacing evaluation when symptoms persist.
Safety, Side Effects, and When to See a Doctor
Insomnia can affect mood, concentration, reaction time, training performance, and overall physical health. Many people improve with consistent behavioral changes, but it is important to recognize when sleep trouble is a warning sign that needs medical evaluation. This section is not a diagnosis guide, but a set of practical guardrails for safety, side effects, and escalation.
When to seek urgent help
Seek urgent medical care right away if you experience chest pain, fainting, suicidal thoughts, or symptoms of mania (for example, a markedly reduced need for sleep with unusually high energy, agitation, impulsive decisions, or risky behavior). Also treat severe shortness of breath during sleep or waking up gasping as urgent, especially if it is new, severe, or paired with dizziness or chest symptoms. Another urgent safety trigger is significant daytime sleepiness that affects driving or operating machinery, since microsleeps can be dangerous even if you feel you are “pushing through.”
When to schedule a routine appointment
Book a routine appointment if insomnia persists despite structured effort (for example, you have consistently tried sleep scheduling, stimulus control rules, or a wind-down routine and still struggle), if daytime functioning is impaired, or if symptoms are worsening over time. Also schedule evaluation if you suspect sleep apnea or another underlying cause. Clues include loud snoring, witnessed breathing pauses, morning headaches, dry mouth on waking, or excessive daytime sleepiness. Pregnancy-related sleep concerns are also a reason to speak with a clinician, since safety guidance for supplements and devices can change based on individual factors.
Medication and supplement safety
If you use prescription sleep medications, use them only with clinician guidance, at the lowest effective dose, for the shortest duration, with reassessment. Many sleep medications can cause next-day impairment, and some carry risks such as tolerance, dependence, falls in older adults, or complex sleep behaviors (for example, unusual behaviors during sleep). Do not mix sedative medications with alcohol or other sedatives.
Supplements can also carry risk. Even commonly used options may interact with medications, and side effects can happen. If you notice adverse effects, stop and discuss with a clinician or pharmacist, especially if you are managing other health conditions.
Be cautious with antihistamines used as sleep aids. They may create short-term drowsiness but can lead to tolerance and an anticholinergic burden (dry mouth, constipation, urinary retention, confusion), particularly in older adults. They are not a long-term strategy, and they can worsen daytime grogginess.
How to prepare for an appointment
Bring a 2-week sleep diary, a list of medications and supplements, and a short symptom log that notes sleep onset time, awakenings, wake time, naps, caffeine/alcohol use, and daytime impact. This gives a clinician enough detail to distinguish patterns and recommend the safest next step.
Products and routines can support sleep management, but they do not replace medical or mental health care when red flags appear or functioning is significantly impaired.
Evidence Snapshot: What Works Best for Chronic Insomnia
Evidence strength varies by approach, and chronic insomnia tends to respond best to strategies that change sleep-driving behaviors over time rather than relying only on short-term symptom relief.
High evidence (most supported for chronic insomnia)
-
CBT-I (Cognitive Behavioral Therapy for Insomnia): strongest overall support for long-term improvement
-
Core behavioral levers often used within CBT-I, including stimulus control and sleep restriction therapy (time-in-bed management)
Moderate evidence (helpful for specific situations or short-term use)
-
Prescription sleep medications: can improve sleep quickly for some people, but are generally best used short-term with clinician guidance due to safety and dependency risks
-
Melatonin: most useful for circadian-related issues (such as delayed sleep timing or jet lag) rather than as a strong sedative
Supportive foundation (helpful, but rarely sufficient alone for chronic insomnia)
Limited / emerging or adjunct support (may help as part of a broader plan)
Durability and safety notes: CBT-I is typically more durable than medication-based approaches, and behavioral strategies generally have the lowest side-effect burden compared with pharmacologic options.
Best Insomnia Treatments FAQs
What are the best insomnia treatments for most people?
For chronic insomnia, CBT-I is widely recommended. For stress-related sleep difficulty, combining relaxation training, consistent sleep habits, and supportive tools such as Pulsetto can help improve sleep readiness.
Is CBT-I better than sleeping pills for chronic insomnia?
CBT-I is often preferred for chronic insomnia because it addresses behavioral patterns and may have longer-lasting effects, while medications are usually recommended short-term.
How long does CBT-I take to work?
Many programs run 4-8 weeks. Some improvement may occur earlier, but consistency is important for durable change.
Which prescription sleep medications are commonly used and what are the risks?
Common categories include DORAs, Z-drugs, and certain antidepressants. Risks may include next-day impairment, dependence, and interactions. Clinician guidance is essential.
Does melatonin work for insomnia, and when should you take it?
Melatonin is most helpful for circadian timing issues. It is typically taken 1-3 hours before desired bedtime and should be used cautiously with medical guidance when needed.
When should insomnia be evaluated for sleep apnea or another medical cause?
If loud snoring, daytime sleepiness, morning headaches, or persistent symptoms occur, medical evaluation is recommended to rule out underlying contributors.

























































